The COVID-19 pandemic poses a serious health threat to the world population. In response, governments are implementing a variety of new policies including self-quarantine, self-isolation and social distancing. While medically necessary to limit spread, these new social policies can disrupt many of the stabilizing factors in our lives which support mental health.
One of the most important brain systems contributing to daily wellbeing is the body’s internal biologic clock. These clocks keep our body and our behavior synchronized with the 24-hour cycle of light and dark. Predictable daily schedules and regular routines help to keep the body clock running smoothly. When our body clocks run smoothly, we feel better. Research shows that disrupted body clocks are associated with many physical and mental health conditions, including depression, diabetes, obesity, and cancer.
When faced with major upheavals in our lives—such as those caused by the COVID 19 pandemic–our body clocks have much more difficulty re-establishing regular biologic rhythms. Absent the normal social routines of work, childcare, and socializing, the biological clock system may be confused or challenged. As a result, we may experience negative physical symptoms similar to jet lag such as disturbed sleep, appetite, energy and mood.
If you have a mood disorder such as depression or bipolar disorder, research suggests that you have a sensitive body clock. Your body clock is more prone to losing track of time when the environment is disturbed, and a disrupted body clock may lead to mood episodes. Paying attention to routines may be especially important during times of stress to keep your body clock regular and your mood stable.
Helping your body clock to stay on track during major life disruptions such as the COVID 19 pandemic may help you feel better. Here are some easy tips for improving the regularity of your daily routines, even when nothing about your life feels regular.
Self-management Strategies for Increasing Regularity of Daily Routines
• Set up a routine for yourself while you are in quarantine or working from home. Routines help stabilize body clocks • Get up at the same time every day. A regular wake time is the most important input for stabilizing your body clock • Make sure you spend some time outdoors every day, especially in the early morning. Your body clock needs to “see” light in the morning to know “when” it is. • If you can’t go outside try to spend at least 2 hours next to a window, looking into the daylight, and focusing on being calm. • Set times for a few regular activities each day such as home tutoring, telephone calls with a friend, or cooking. Do these activities at the same time each day.
• Exercise every day, ideally at the same time each day. • Eat meals at the same time every day. If you’re not hungry, at least eat a small snack at the prescribed time. • Social interactions are important, even during social distancing. Seek out “back and forth” social interactions where you share thoughts and feelings with another person in real time. Videoconferencing, telephone or even real-time text-messaging is preferred to scrolling through messages. Schedule these interactions at the same time every day. • Avoid naps during daylight hours, especially later in the day. If you must nap, restrict them to 30 minutes. Napping makes it hard to fall asleep at night. • Avoid bright light (especially blue light) in the evening. This includes computer screens and smartphones. Blue spectrum light suppresses the hormone that helps us sleep. • Stick to a consistent sleep and wake time that fits your natural rhythms. If you are a night owl, it’s ok to stay up a little bit later and get up a little bit later than others in the household. Just make sure you go to sleep and get up at the same time every day.
Medication alone is rarely the complete answer for individuals with bipolar disorder. Responses are incomplete, prevention is imperfect, lingering symptoms remain and adherence to treatment is often a challenge. Substance use, inadequate and irregular sleep schedules, fluctuations in activity, and poor regulation of emotional stimuli can also contribute to limiting the effectiveness of medications. For these and other reasons, psychological therapies have been investigated as adjuncts in the overall management of this illness.
History and Development of Psychoeducation
The first psychological efforts to address bipolar disorders
were intensive, psychoanalytic therapies conducted during the first half of the
20th century. Occurring at a
time when there were no other empirically proven treatments, these psychoanalytic
therapies that were designed for more common emotional problems did not show
promise in altering the course of manic-depressive illness. Following this, cognitive behavioral therapy
and family focused therapy were two of the first, standardized psychological
interventions evaluated in the treatment of bipolar disorders.
Psychoeducational therapy for bipolar disorders arose in the
late 1980’s. It occurred in reaction to
the traditional medical model prevalent prior to that time. That medical model was characterized as
paternalistic and biomedical, viewing illness as the sole cause of suffering
and doctors and their medications as the sole source of treatment. The patient’s understanding of their
condition was not seen as important and patients were not active participants
in their treatment. Enter
psychoeducation.
Psychoeducation was a radical break from the medical
authoritarianism of the early 20th century. Based on the premise that knowledge is power,
its goal was to provide information to patients about their illness. Early reports from the Netherlands suggested
that this approach could improve self-confidence and lessen the isolation and
stigma that mental illness so often confers.
Matters that we take for granted today.
A Current Model of Psychoeducation
These early efforts paved the way for later, more refined
psychoeducational therapies. Combining
information provision with elements of proactive self-management and social support,
Colom and colleagues in Barcelona developed the first, modern psychoeducational
therapy for bipolar disorders 1. It consisted of 21 group sessions, each
focusing on one of five major areas:
Awareness
of the disorder
Medication
adherence
Avoiding
substance abuse
Early
detection of new episodes
Regular
habits and stress mgmt.
Here is a list of the 21 topics covered in each of the above
five areas:
Research Findings
Designed as a maintenance treatment to prevent relapse among
stable, euthymic patients, the first study of this modality was wildly
successful, showing dramatically reduced relapse rates for manic, depressive
and mixed mood episodes over the two-year time period of the study (see graph
below).
A follow-up study on the same cohort of subjects, tested
three years later showed that the benefits not only persisted but – in some
cases (e.g., manic relapse) – had increased over time 2. Incredible results!
As a consequence of these foundational reports and some
other replication studies, psychoeducation was adopted by several international
treatment guidelines as a first-line, adjunctive treatment for all individuals
with bipolar disorder who were in stable remission. But then, as always, the story got a little
more complicated.
In 2015, Kirsten Bond and colleagues from the UK, conducted
a careful systematic review of all studies done on psychoeducation 3. A systematic review is a prescribed, formal
method of scouring the entire scientific literature on all studies in a given
area. It is designed to be thorough,
clear, transparent and objective, attempting to avoid the biases that can
plague individual studies. Combing
through an initial search of almost 1600 articles, the authors found only 8
that met their strict inclusion criteria.
The upshot? When pooling the
results of these eight studies, they confirmed that psychoeducation
significantly reduced relapse into any mood episode, especially manic
relapse. Their finding on prevention of
depressive relapse were more equivocal and were only significant when examining
group-based (vs. individual) psychoeducation.
Two more caveats. First, they
noted that there was considerable variability in the treatment formats used in
the studies; some used individual psychoeducation, others used group. The length of treatments varied between as
few as 2 and as many as 21 sessions. This
heterogeneity introduced uncertainty to the overall findings. Second, the results from the initial studies
by Colom’s group in Barcelona were outliers; they were much more significant
than all the other studies. When those
were removed, the efficacy of psychoeducation in the remaining studies was cut
in half. Further sobering news
followed.
Prompted by the caution of this systematic review and a
relative absence of independently conducted replication research, Richard
Morriss and colleagues designed a careful, randomized, single-blind study of
psychoeducation vs unstructured peer support groups 4. As with all research in this area, the
psychoeducation and control groups were adjunctive to standard medication
therapy. Their design, however, differed
in two significant respects from the original research of the Colom group: First, instead of requiring six months of
mood stability (euthymia), they required only 4 weeks; second, while Colom
excluded patients with any comorbid disorders (eg, anxiety problems, substance
abuse, etc..), these authors allowed almost anyone to enter their study. This creates more of a real-world examination
of the treatment. Apart from these
distinct inclusion and exclusion criteria, the treatment was exactly the same
as the Colom group: 21 group
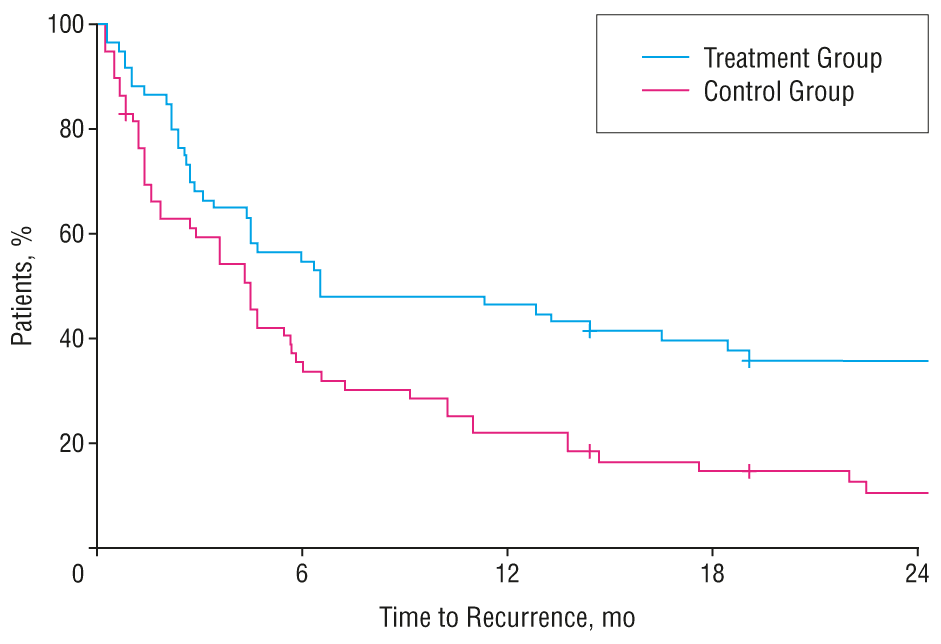
sessions. The primary outcome measured
was time to relapse over the almost two years of the study. The main results are shown below:
The graph shows survival curves of the two groups,
representing the percentage of each group that “survived” or avoided relapse
over the 92 weeks of the study. As you
can see, the curves are almost identical, indicating no significant difference
between the psychoeducation and control arms of the study. Yikes!
How do we explain the differences between the initial, dramatically
positive results for this intervention and the later, more cautious systematic
review and this recent, negative study? And what does this mean for the status
of this first-line psychological treatment for bipolar disorders?
Synthesis and Conclusion
We suggest that the way to reconcile these contradictory
findings lies in the different entry criteria and cohorts used in the initial
vs. the later studies. Colom’s group set
a very high bar for participation in their research: subjects needed to be euthymic for six months
and free of other major psychiatric disorders.
This creates an ultra-rarefied cohort, one that would not generalize
well to the real world where patients typically have several disorders at once
and are rarely free of symptoms for extended periods of time. If this difference accounts for the disparate
findings, this suggests that psychoeducation might be more useful early in the
course of their illness and in those patients without significant
comorbidity. Here’s our take home on
this.
Psychoeducation is an intervention designed to help individuals with bipolar disorders better understand their illness and their ability to manage it.
The weight of research on psychoeducation supports a maintenance effect of preventing episode relapse.
This relapse prevention effect is probably more pronounced among patients who have not had high numbers of prior episodes or multiple other existing mental health disorders.
While perhaps not the glowing success that the foundational studies suggested, in terms of providing patients with a coherent way of understanding and managing the tumultuous course of their mood states, psychoeducation remains the best game in town. We believe it should remain as part of the ‘core curriculum’ of all treatment efforts.
John Gottlieb
1. Colom
F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group
psychoeducation in the prophylaxis of recurrences in bipolar patients whose
disease is in remission.[see comment]. Arch
Gen Psychiatry. 2003;60(4):402-407.
2. Colom F, Vieta E, Sanchez-Moreno J,
et al. Group psychoeducation for stabilised bipolar disorders: 5-year outcome
of a randomised clinical trial. Br J
Psychiatry. 2009;194(3):260-265.
3. Bond K, Anderson IM. Psychoeducation
for relapse prevention in bipolar disorder: a systematic review of efficacy in
randomized controlled trials. Bipolar
Disord. 2015;17(4):349-362.
4. Morriss R, Lobban F, Riste L, et al.
Clinical effectiveness and acceptability of structured group psychoeducation
versus optimised unstructured peer support for patients with remitted bipolar
disorder (PARADES): a pragmatic, multicentre, observer-blind, randomised
controlled superiority trial. The lancet
Psychiatry. 2016;3(11):1029-1038.
The brain is the seat of the mind – this fundamental
governing principle has driven the study of the biological causes of mental
illness for the past century and beyond. For years, scientists have studied the
inner workings of our brains in order to better understand mental illness, its
causes, and potential treatments. Initial efforts in this area focused on the
gross anatomy of the brain and the study of large brain regions. With the
discovery of effective psychotropic medications, this gave way to investigation
of neurotransmitters such as serotonin and dopamine, and their role in mental
illness. In recent history, the focus of scientific investigation has shifted
towards the study of brain networks, and the expression of the genes they
contain.
Five years ago, I reviewed some of the scientific literature on the neuroplasticity model of depression – a fascinating new way to think about mood disorders. Departing from the earlier, monoamine-based ideas – too little serotonin or dopamine – this model suggests that depressive states are associated with a reduction in the brain’s ability to change in response to experience. In my earlier review of neuroplasticity, I described how our brains are not fixed organs but are instead constantly changing in response to novel information and new learning. These changes involve strengthening or weakening of synaptic connections along with growth or shrinkage of neurons. In health, there is a constant growth, sculpting and refinement of neural pathways. This plasticity becomes impaired in depression: the brain becomes less malleable, there is reduced new learning and people become trapped in despair. The neuroplasticity model is a radically different way of thinking about mood disorders. What follows is an update on research on this area, which has focused on several major developments. These include the following: 1) investigations of brain plasticity based on visual evoked potentials (VEPs); 2) the use of learning and memory tests to evaluate structural change in the CNS and; 3) emerging research on the impact of antidepressants on neuroplasticity.
Ketamine is a medication that was developed in the 1960s. It was approved as an anesthetic agent for use during medical and surgical procedures by the Food and Drug Administration (FDA) in 1970. Since that time, it has been used primarily as a medication to induce anesthesia (loss of consciousness), and has been used in the management of chronic pain conditions. It is generally given to patients through an IV, but can also be given in inhaled and oral forms. Ketamine is also a drug of abuse that is used illicitly in the United States, and can lead to addiction.
Patients with bipolar disorder often manifest cognitive disturbances during acute manic, depressive, and mixed states which include difficulties with attention, concentration, planning and memory. It may come as a surprise, though, to learn that cognitive deficits can persist into euthymia – a state of relative mood stability. Indeed, approximately 40 % of euthymic bipolar patients show evidence of cognitive impairment (1,2) involving attention, executive function (i.e. planning and organization, cognitive flexibility and set-shifting, and working memory), verbal memory, processing speed and visual memory (3,4). Patients with bipolar I and bipolar II disorder appear to have a similar pattern of deficits (4). The purpose of this brief review is to identify cognitive deficits that help distinguish bipolar disorder from other disorders of mood, memory, and executive functioning. An improved understanding of these deficits will help clinicians tailor their treatment interventions to address the individual needs of patients.
If you’ve come to this website and are reading this article, the odds are good that you or someone that you know has been diagnosed with a mood disorder. You might be seeking more information about emotional illnesses. But before diving into any of the numerous areas of research presented at our site, what if we pause and ask a very basic but important question: what are moods? We use this term all the time, but do we truly understand what they consist of and why we experience them? Even more fuzzy, what about the term, ‘affects’? We specialize in the treatment of ‘affective illness’ here, but what is an affect and how is it different from a mood? This brief review will summarize a generally accepted concept of emotions, describe their composition and functional purpose and present current research in this area. To start, let’s begin by taking a look at how these terms are currently used in clinical practice.
The Lithium Membrain by Anne Naylor. Lithium coursing through veins in the brain (blue) provides mood stability by acting as a membrane that prevents the effects of the various faces of the illness (circles) on the brain (neural networks).
(Copied with permission from: Anne Naylor and Malhi, G. S. “Lithium therapy in bipolar disorder: a balancing act?” The Lancet 2015386(9992): 415-416.)
In my previous blog, I described “temperament” as one’s constitutionally determined way of responding emotionally to the world and introduced Akiskal’s five affective temperaments: Depressive, Hyperthymic, Cyclothymic, Irritable, and Anxious (1). Akiskal’s conceptualization of temperament begins with endophenotypes; that is, the outward expression of a gene or trait. These descriptive endophenotypes provide the scaffolding from which one learns about the underlying processes involved in their formation and evolution. This approach to studying personality and temperament can best be described as “top-down” – start with what you observe and go from there, from macro to micro. Another example of the “top-down” view includes the work of Eysenck, who described three “dimensions” of human personality: Neuroticism (N), Psychoticism(P), and Extroversion (E) (2). Still another example is that of Cloninger, who described temperament using the following terms: novelty seeking, harm avoidance, reward dependence, persistence, self-directedness, cooperativeness, and self-transcendence (3).
Emotional expression, or “affect,” covers a range of temporal domains. There are “emotions,” moment-to-moment fluctuations which, while intensely experienced, come and go within minutes. When a given emotional state lasts longer – hours, days, or months – it is described as “mood.” Finally, there is “temperament,” a lifelong emotional disposition considered to be part of one’s constitutional makeup (1). When temperament manifests as “affective” – that is to say, appears as a similar but less severe variant of a disordered mood state – things start to get interesting.